
Vitamin K & Warfarin Stabilizer Calculator
Your Current Situation
INR Stability Analysis
INR Stability:
Important Note: This calculator provides educational insights based on clinical research. Always consult your healthcare provider before making any changes to your warfarin therapy.
Staying on warfarin is already complicated. You’ve got to remember your dose, avoid certain foods, get your blood tested regularly, and hope your INR doesn’t swing too high or too low. But what if the problem isn’t your warfarin dose - it’s your vitamin K intake? For many people, the real culprit behind wild INR swings isn’t missing a pill or eating too much broccoli. It’s inconsistent vitamin K levels. And there’s a simple, low-cost fix that’s quietly helping thousands: vitamin K supplements.
Why Your INR Keeps Fluctuating
Warfarin works by blocking vitamin K’s role in making clotting factors. That’s why it thins your blood. But here’s the catch: your body needs vitamin K for other things too - like bone health and artery function. So even if you’re not eating a lot of leafy greens, your body still uses vitamin K daily. The problem? Your intake varies. One day you eat a salad, the next you skip it. One week you take a multivitamin with K, the next you don’t. That inconsistency throws off your warfarin balance. Your INR (International Normalized Ratio) measures how long it takes your blood to clot. For most people on warfarin, the target is between 2.0 and 3.0. If it drops below 2.0, you’re at risk for clots. Above 4.0, you’re at risk for serious bleeding. About half of all warfarin users experience INR levels outside this range at least once every few months. That’s not normal. It’s not just bad luck. It’s often because vitamin K levels are all over the place.How Low-Dose Vitamin K Helps
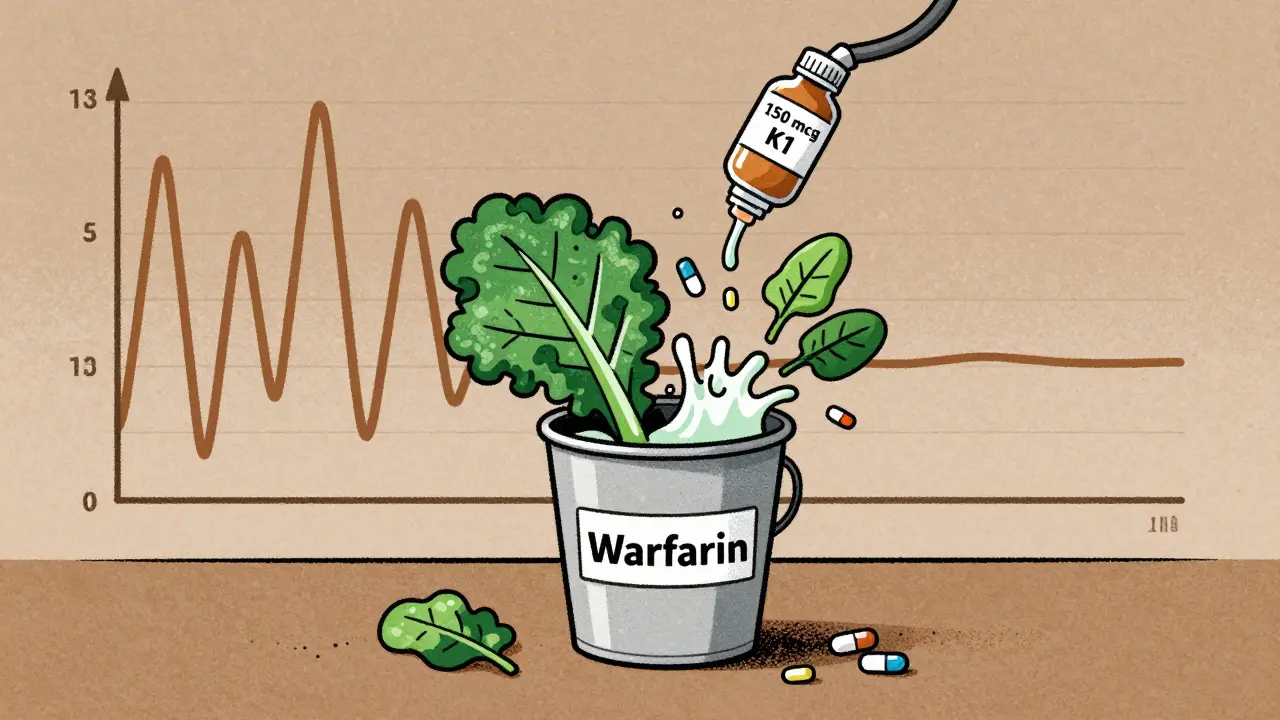
Research from 2007 showed something surprising: people with unstable INRs were getting only about 109 micrograms of vitamin K per day. People with stable INRs? Around 293 micrograms. That’s a huge difference. The fix? Give everyone the same amount - every day. The standard dose used in clinical trials is 150 micrograms of vitamin K1 (phylloquinone) taken orally once daily. That’s about 1.5 times the recommended daily intake for women, and slightly above for men. It’s not a huge amount. It’s not a magic bullet. But it’s enough to smooth out the daily ups and downs in your vitamin K supply. Think of it like filling a bucket with a leaky hose. Warfarin is the leak. Vitamin K from food is the water - sometimes you get a big splash, sometimes a drip. Adding a steady drip of vitamin K from a supplement keeps the water level more consistent. That means your INR doesn’t spike or crash as often.What the Studies Show
A 2016 Canadian trial followed 190 people on warfarin who had unstable INRs. Half took 150 mcg of vitamin K daily. The other half took a placebo. After six months, both groups had similar average INR levels. But here’s the key: the vitamin K group had far fewer dangerous spikes. Extreme INR values (below 1.5 or above 4.5) dropped from 9.4% of tests to just 5.4%. That’s a 4% absolute reduction - meaning roughly one fewer dangerous INR every two months. Another study found that 54% of patients on vitamin K supplements achieved stable control, compared to only 21% in the placebo group. That’s not just statistical. That’s real life. One patient, a 68-year-old man with a mechanical heart valve, went from 42% time in range to 71% after starting vitamin K. His warfarin dose only needed two adjustments over six months - down from 17 in the previous 18 months. But here’s the catch: vitamin K doesn’t always improve your average INR. It doesn’t make your TTR (Time in Therapeutic Range) magically jump from 50% to 80%. What it does is reduce the extremes. And for people who’ve had strokes or bleeds because of INR swings, that’s everything.Who Should Consider It
This isn’t for everyone. If you’re stable on warfarin - your INR stays in range, you rarely need dose changes - you don’t need it. But if you’re one of these people, it’s worth talking to your doctor:- You’ve had three or more INR readings above 4.0 or below 1.5 in the last six months
- Your TTR (Time in Therapeutic Range) is below 65%
- You eat a varied diet but still can’t get your INR steady
- You’re on warfarin because of a mechanical heart valve, antiphospholipid syndrome, or severe kidney disease - not just atrial fibrillation
What You Need to Know Before Starting
You can’t just walk into a pharmacy and start taking vitamin K without supervision. Here’s how it actually works:- Your doctor checks your recent INR history. If you’ve had consistent instability, they may suggest a trial.
- You start 150 mcg of vitamin K1 daily - usually one tablet, often sold as a generic supplement.
- You continue your regular warfarin dose - do not change it yet.
- Your INR is checked weekly for the first month. It may drop a bit as your body adjusts. Your doctor might increase your warfarin by 0.5 to 1.5 mg to compensate.
- After one to two months, your INR should stabilize. If it doesn’t, you stop.
Cost, Safety, and What’s Available
A bottle of 100 tablets of 150 mcg vitamin K1 costs about $8 at most pharmacies. That’s less than 0.5 cents per day. It’s cheaper than your morning coffee. And it’s safe. The European Food Safety Authority says you’d need to take 10,000 times this dose daily to risk toxicity. There’s no evidence of liver damage, kidney issues, or interactions with other medications. You can buy vitamin K1 (phylloquinone) as a standalone supplement. Avoid K2 (menaquinone) - it’s not studied for this use. Look for products that say “vitamin K1” or “phylloquinone.” Some multivitamins contain K1, but the dose is usually too low (5-20 mcg) to help. You need the full 150 mcg.What Doesn’t Work
Vitamin K supplements won’t help if:- You’re inconsistent with your warfarin dose
- You eat huge amounts of vitamin K - like a whole head of kale every day
- You’ve recently had a blood clot or are on dialysis without close monitoring
- You’re not willing to keep getting your INR tested

Ian Long
January 8, 2026 AT 07:38
Bro, I’ve been on warfarin for 7 years and my INR was all over the place until I started the 150 mcg K1. No more panic calls to the clinic. My doctor was skeptical, but now he’s the one recommending it. Cheap, simple, and it actually works. Stop overcomplicating it.
Matthew Maxwell
January 9, 2026 AT 17:54
While the anecdotal evidence may seem compelling, this approach lacks rigorous, large-scale validation. The 2016 Canadian trial you cite had a sample size of 190-far too small to establish clinical guidelines. Furthermore, the mechanism by which vitamin K stabilizes INR without altering warfarin pharmacokinetics remains biologically implausible without a controlled metabolic pathway. This is not medicine-it’s nutritional superstition dressed in peer-reviewed clothing.
Lindsey Wellmann
January 11, 2026 AT 14:28
OMG I JUST STARTED THIS AND MY INR IS ACTUALLY STABLE?? 🥹💖 I was crying in the lab last week because my INR was 4.8… now it’s 2.7 and I didn’t even change my warfarin! I told my nurse and she looked at me like I was a genius 😭✨ #VitaminKIsMagic #WarfarinWarrior
Meghan Hammack
January 11, 2026 AT 19:00
You’re not alone. I was so scared to try this because I thought supplements were risky. But after three bad INRs in a row, I said ‘screw it’ and started the 150 mcg. My doctor adjusted my warfarin up a little, and boom-no more hospital visits. It’s not a cure, but it’s the first thing in years that actually helped me sleep at night. You got this. 💪
RAJAT KD
January 13, 2026 AT 10:52
150 mcg daily is correct. Vitamin K1, not K2. Avoid multivitamins-they contain 10 mcg, useless. Monitor INR weekly for first month. Doctor must adjust warfarin. This is evidence-based. Done.
Chris Kauwe
January 15, 2026 AT 07:20
Let’s be real-this isn’t about vitamin K. It’s about the collapse of the American healthcare system. We’ve outsourced biological regulation to a pharmaceutical-industrial complex that profits from instability. Vitamin K supplementation is a grassroots reclamation of physiological autonomy. The system fears consistency because consistency undermines profit. This is the quiet revolution they don’t want you to know about.
Alicia Hasö
January 16, 2026 AT 00:30
If you’re reading this and your INR is still a rollercoaster-please, talk to your anticoagulation team. This isn’t a miracle, but it’s one of the few things that actually gives people back control. You’re not failing. Your body isn’t broken. You just need the right tool. And sometimes, that tool is a $8 bottle of K1. You deserve stability. Don’t give up.
Ashley Kronenwetter
January 17, 2026 AT 12:36
While the clinical data appears promising, the potential for unmonitored self-administration poses significant risk. Vitamin K supplementation alters warfarin pharmacodynamics and requires precise titration under professional supervision. I strongly advise against initiating this regimen without documented INR history and physician oversight. Patient safety must remain paramount.
Aron Veldhuizen
January 18, 2026 AT 17:47
Actually, this is all just a placebo effect fueled by confirmation bias. If you’re taking 150 mcg of K1, you’re essentially giving your body a consistent baseline-but so is eating one spinach salad every day. The real issue? You’re not tracking your food intake properly. The supplement is just a crutch for people who refuse to keep a food diary. And let’s be honest-most of you don’t even know what phylloquinone is. You just read ‘vitamin K’ and thought it was magic.