When your skin breaks out in red, itchy patches, it’s easy to assume it’s just eczema-or psoriasis. But these two conditions look similar on the surface and are often confused. The truth? They’re fundamentally different diseases with distinct visual signatures. Getting it right matters because treating eczema like psoriasis (or vice versa) can make things worse. Here’s how to tell them apart just by looking at the rash.
Location Tells the Story
Where the rash shows up is one of the biggest clues. Eczema loves the flexural areas-the skin folds. Think inside your elbows, behind your knees, the creases of your wrists, and around your neck. In babies, it often hits the cheeks and scalp. This pattern is so consistent that 92% of adult eczema cases involve the inner elbows, and 89% show up behind the knees. Psoriasis, on the other hand, prefers the extensor surfaces-the outer parts of your body. You’ll commonly see it on the outside of your elbows, the front of your knees, your scalp, lower back, and even your nails. A 2020 JAMA Dermatology study found that 88.6% of psoriasis cases affected these areas, while only 9.1% of eczema cases did. If you have thick, scaly patches on your scalp or elbows, it’s far more likely to be psoriasis.Shape and Borders: Blurry vs. Sharp
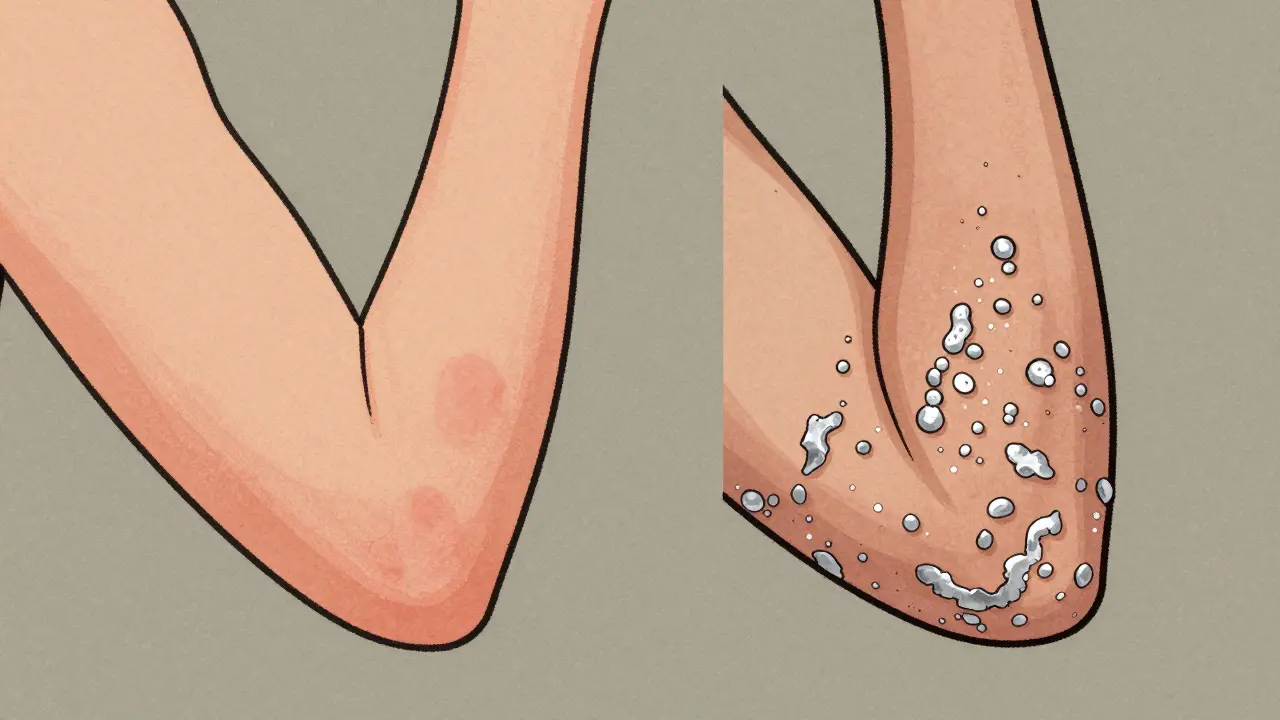
Eczema rashes usually have fuzzy, poorly defined edges. They blend into the surrounding skin, making them look patchy and irregular. The inflammation doesn’t stay in one neat box-it spreads softly, like a watercolor stain. Psoriasis is the opposite. Its plaques have crisp, sharp borders, almost like they were drawn with a ruler. These raised, well-defined patches stand out clearly against healthy skin. That contrast is one reason psoriasis often feels more “visible” to patients. In fact, 76% of people with psoriasis describe their rash as looking like “armor plating” because of how sharply it stands out.Texture and Scaling: Oozing vs. Silvery
This is where the difference becomes unmistakable. Eczema skin is often thin, dry, and cracked. In its acute phase, it can weep, ooze, or even crust over. Think of it like a sunburn that’s broken open-raw, tender, and sometimes wet. Chronic eczema leads to lichenification, where the skin thickens from constant scratching, but the surface stays rough, not scaly. Psoriasis is dry. Really dry. It builds up thick, silvery-white scales that cling tightly to the skin. These aren’t flaky like dandruff-they’re dense, like pieces of paper glued on. When you scrape them off (a trick dermatologists use), you might see tiny drops of blood underneath. That’s called the Auspitz sign, and it’s almost never seen in eczema. A 2023 British Journal of Dermatology study confirmed that 78% of psoriasis lesions had visible scaling, compared to only 32% of eczema cases.
What About Skin of Color?
Most textbooks show eczema and psoriasis on fair skin. But that’s not the whole picture. On darker skin tones, the colors change. Eczema doesn’t always look red. Instead, it can appear as dark brown, purple, or ashen patches with subtle scaling. Psoriasis turns violet or deep brown, and the scales may look grayish instead of silvery. A 2021 JAMA Dermatology study found that misdiagnosis rates for both conditions are 35% higher in people with Fitzpatrick skin types IV-VI. Why? Because many doctors were never trained to recognize these variations. A 2023 survey of 500 dermatologists showed 68% felt underprepared to diagnose these rashes on darker skin. That’s why visual guides now include photos of all skin tones-something the Global Registry of Skin of Color Dermatology is pushing hard for since 2024.Nail Changes and Other Clues
Psoriasis doesn’t stop at the skin. About half of people with psoriasis get pitted nails-tiny dents like someone tapped them with a pin. In 80% of cases with nail involvement, the nail lifts from the bed (onycholysis). These changes are rare in eczema. You might see ridges or discoloration in severe eczema, but never true pitting. Another key difference? The Koebner phenomenon. If you scratch or injure your skin and new lesions appear exactly where the injury happened, it’s more likely psoriasis. This happens in 25-30% of psoriasis patients but is rare in eczema.How Patients Describe the Difference
Real people describe these conditions in ways that match the science. On eczema forums, 87% say their skin looks “raw,” “weepy,” or “cracked open.” On psoriasis forums, 89% mention “thick, silvery scales.” Reddit users in r/eczema talk about constant itching and bleeding from scratching. Those in r/Psoriasis describe feeling like their skin is “armored” and “stuck with glue.” The emotional impact is different too. People with psoriasis often say their condition is instantly noticeable. Eczema patients say theirs blends in-until it flares and starts leaking.
Simple Tests You Can Try
You don’t need a dermatoscope to spot the difference. Try this at home: gently scrape the edge of a patch with a clean glass slide or credit card. If thick, silvery scales lift off and you see pinpoint bleeding underneath, it’s likely psoriasis. If the skin just flakes lightly without bleeding, it’s probably eczema. Also, track the pattern. Eczema flares and fades with triggers-hot showers, stress, soap, dry air. Psoriasis stays stubborn. Once a plaque forms, it doesn’t vanish overnight. It may shrink slowly, but it won’t disappear just because you moisturize.What About AI and Apps?
New AI tools like the DermAI Psoriasis/Eczema Classifier (FDA-approved in January 2024) can analyze smartphone photos with 85% accuracy. But here’s the catch: they’re 22% less accurate on darker skin tones. That’s because most training data came from lighter skin. No app replaces a trained eye. Even the American Academy of Dermatology warns that digital tools should only support-not replace-clinical judgment.Why This Matters
Misdiagnosis happens in 15-20% of cases. If you have psoriasis and use steroid creams meant for eczema, you might trigger a rebound flare. If you have eczema and take psoriasis biologics, you could waste time, money, and risk side effects. Getting the right diagnosis means getting the right treatment. The bottom line? Look at the location, the borders, the texture, and the scale. Eczema: soft, weepy, inside the creases. Psoriasis: thick, scaly, outside the creases. When in doubt, see a dermatologist. But now you know what to look for.Can eczema and psoriasis occur at the same time?
Yes, it’s possible-though uncommon. Some people have both conditions, especially if they have a strong family history of autoimmune or allergic skin issues. In these cases, one condition might dominate in certain areas while the other appears elsewhere. A dermatologist can distinguish them by examining each lesion individually and may use biopsy if needed.
Does scratching make psoriasis worse?
Scratching doesn’t cause psoriasis, but it can trigger new lesions through the Koebner phenomenon-where trauma to the skin leads to new plaques forming in the same spot. It also worsens itching and inflammation, making the condition harder to manage. For eczema, scratching is a direct symptom of the itch-scratch cycle, which fuels the flare.
Can moisturizers cure either condition?
No, moisturizers don’t cure either. But they’re essential for managing both. For eczema, thick ointments (like petroleum jelly) restore the skin barrier and reduce flares. For psoriasis, moisturizers help soften scales and reduce cracking. However, neither condition responds to moisturizer alone. Eczema often needs topical steroids or calcineurin inhibitors; psoriasis may require phototherapy, biologics, or systemic drugs.
Why does psoriasis have silvery scales?
Psoriasis is caused by an overactive immune system that speeds up skin cell production. Normal skin sheds every 28 days. In psoriasis, skin cells reach the surface in just 3-5 days. They pile up before they have time to shed, forming thick, layered plaques. The silvery scales are dead skin cells trapped on top. Eczema doesn’t have this rapid turnover-it’s driven by barrier dysfunction and inflammation, not excess cell growth.
Is psoriasis contagious?
No, absolutely not. Neither eczema nor psoriasis is contagious. You can’t catch it from touching someone, sharing towels, or being near them. Both are immune-related conditions with genetic triggers, not infections. Misunderstanding this leads to stigma, especially for people with visible plaques.
Matt Alexander
March 5, 2026 AT 20:25
So simple: eczema = wet, itchy, creases. Psoriasis = dry, scaly, outside edges. I’ve had both and this nailed it.
Moisturizer helps both but doesn’t fix either. You need real treatment.
Stop guessing. See a derm.
Gretchen Rivas
March 5, 2026 AT 20:28
I’m dark skin and this article changed everything for me.
My eczema never looked ‘red’-it was deep purple. No one ever told me that.
Thank you for including skin of color. Finally.
Milad Jawabra
March 7, 2026 AT 12:53
Y’all are overcomplicating this. Eczema = your skin is crying. Psoriasis = your skin is screaming with armor.
Stop googling and go see someone who’s seen 1000 of these.
I’ve been there. You’re not alone. But you ARE late.
Go. Now. Seriously. Your skin will thank you.
-Your friendly neighborhood dermatology hype-man 😤
Mike Dubes
March 7, 2026 AT 23:13
So psoriasis is like your skin’s on turbo mode growing cells? That makes sense.
I thought it was just ‘bad dryness’ till I saw the scales lift and bleed.
Wtf that’s wild.
Also yeah moisturizer’s not a cure but damn it helps with the crackin’.
Just saying.
And no it’s not contagious lol why do people still think that??
Sharon Lammas
March 9, 2026 AT 21:17
It’s strange how we assign so much meaning to skin.
Eczema feels like vulnerability. Psoriasis feels like defiance.
Both are battles, but one is whispered, the other roared.
I wonder if the body’s language mirrors the soul’s silence or its scream.
Either way, we owe people with these conditions more than just diagnostics.
We owe them dignity.
And that starts with seeing them-really seeing them.
Stephen Vassilev
March 11, 2026 AT 16:08
Have you considered that this entire classification is a pharmaceutical construct designed to sell creams and biologics?
What if the ‘difference’ is artificially manufactured by dermatology guidelines funded by Big Pharma?
Have you seen the 2024 FDA approval timeline for DermAI?
It was signed by a former AbbVie executive.
And why is there no mention of gut microbiome links?
Are we being manipulated into believing two separate diseases when it’s all just immune dysregulation?
Wake up.
Don’t let them label your skin.
Question everything.
John Cyrus
March 12, 2026 AT 17:39
Anyone who thinks moisturizer fixes eczema is delusional.
You need steroids. Period.
And if you’re using ‘natural remedies’ instead of seeing a doctor you’re endangering your health.
Stop listening to TikTok influencers.
This isn’t a yoga pose.
It’s a medical condition.
Grow up.
John Smith
March 13, 2026 AT 22:31
Yo I got psoriasis on my elbows and let me tell you it feels like someone glued brick dust to my skin.
And yeah the silvery scales? That’s the real MVP.
Try scraping one off with a credit card-BOOM-tiny blood spots.
That’s not a myth. That’s science.
Also I got pitted nails and no one believed me till I showed the pics.
Now I’m the psoriasis king of Reddit.
👑
Helen Brown
March 14, 2026 AT 03:02
Did you know the government tracks skin conditions through the CDC to monitor ‘immunological trends’?
And that the AI tools are trained on data from military hospitals?
Why? Because they’re studying how stress affects skin as a biomarker for PTSD.
They’re not just diagnosing rashes.
They’re mapping your nervous system.
And the ‘skin of color’ section? That’s just to make people feel better.
The real data is locked away.
Trust no one.
Aisling Maguire
March 15, 2026 AT 03:27
My mum had both at once and it was chaos.
One patch on her knee was psoriasis-thick and scaly.
The patch next to it? Eczema-raw and weeping.
She’d mix up the creams and end up worse.
Finally got a derm who looked at each spot like a fingerprint.
That’s the key.
Not the whole arm.
Each lesion.
One by one.
She’s been stable for 3 years now.
Good luck out there, folks. You got this 💪